Back to Fort Fairfield Journal WFFJ-TV Contact Us

![]()
![]() .
.
U.S. FDA & CDC Shared Database Now Shows Over 20,000 COVID ‘vaccine’ Deaths in First Year of Experimental Gene Therapy
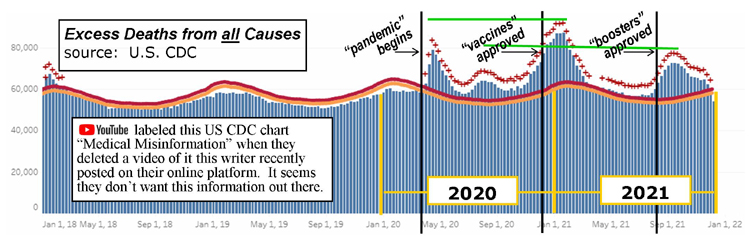
This U.S. CDC chart shows excess deaths from all causes (not just COVID-19) from January, 2018 through present day with each vertical bar representing a week out of the respective year. The red line is the upper threshold of what would be expected for deaths that week. The weeks with the red + signs show excess deaths. This writer overlaid additional timeline data to show in 2021, the two great “surges” in excess deaths followed the initial release of the COVID-19 gene therapy bioweapon shots in December, 2020 and subsequent “boosters” which began in August, 2021. Intriguingly, the excess deaths surges were higher during the 2021 “vaccine” year than they were in the first year of the pandemic when there were no vaccines and no natural immunity to COVID-19 (green lines). Throughout the pandemic, many normal deaths were deliberately mislabeled as “COVID-19” for political purposes and to help market the gene therapy bioweapon shots to the public.
chart: https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm#dashboard
By: David Deschesne
Fort Fairfield Journal, December 29, 2021
As of December 10, 2021 the Vaccine Adverse Event Reporting System (VAERS) shows a total of 20,622 deaths associated with the COVID-19 gene therapy bioweapon shots which began wide-scale implementation in the general population just over a year ago (chart is updated weekly).1
To provide context, this writer researched the VAERS for flu vaccine deaths and found that same database shows all flu vaccines in existence between the years of 2015-2019 only logged a total of 121 deaths over that five year period, or an average of 24 seasonal flu vaccine deaths per year.2
The VAERS is a database maintained by the U.S. Food and Drug Administration (FDA) and Centers for Disease Control (CDC). The database is spontaneous and accepts reports from vaccine manufacturers, healthcare providers, vaccine recipients and others. VAERS is used for detecting signals of potential vaccine safety problems that may be further studied. However, it is a passive surveillance system relying on voluntary submissions and may be subject to over-reporting, under-reporting or bias.
A few years ago, researchers from Harvard University conducted a study of the VAERS and found that only around 10% of all adverse vaccine events get reported to that system which means the numbers may be under-reported by as much as 90%. In the current highly politicized COVID-19 climate, many hospitals and doctors are biased in favor of the experimental ‘vaccines’ and thus don’t consider a COVID ‘vaccine’ death as an actual vaccine death and simply choose not to report it. Also, the U.S. CDC has chosen not to designate a vaccine death if the person died within fourteen days of receiving one of the experimental COVID-19 shots because they don’t consider the person ‘vaccinated’ until 14 days after receiving the shot.3 Ergo, the CDC deceptively calls those vaccine deaths “unvaccinated COVID-19 deaths” thus skewing the numbers in favor of the ‘vaccines.’
Furthermore, research published in the medical journal, Toxicology Reports4 showed CDC data that admitted that the vast majority of deaths from the COVID vaccines occurred within the first 10 days of receiving the COVID shot. All of these deaths are deceptively considered by the CDC as “unvaccinated individuals” so they won’t have to admit a vaccine connection to the deaths.
Researcher Steve Kirsch, Executive Director of the COVID-19 Early Treatment Fund, has analyzed vaccine deaths in the U.S. using CMS data from Medicaid and Medicare. He found there are likely around 41 times more COVID ‘vaccine’ deaths overall than are currently listed in the VAERS.5
Since VAERS can receive reports from vaccine manufacturers and other international sources, looking at the deaths in the U.S. and territories alone that number was 9,136 as of December 3, 2021. If Kirsch’s under-reporting factor of 41 is correct, then the actual real number of U.S. deaths from the COVID-19 gene therapy bioweapon shots may be closer to 374,576. If we add the international deaths reported to VAERS that number could be more than 800,000 COVID ‘vaccine’ deaths as of December 3—most of which simply haven’t been reported to that system.
Given the fluidity of the numbers at the VAERS database, one can find a more concrete view in the CDC’s Excess Deaths statistics which logs actual deaths from all causes (not just COVID) in the U.S. over the years (ref. chart, above).6 The two major surges in excess deaths in 2021 coincided with the initial rollout of the experimental COVID drugs in December, 2020 and the approval of “booster” shots in late summer, 2021.
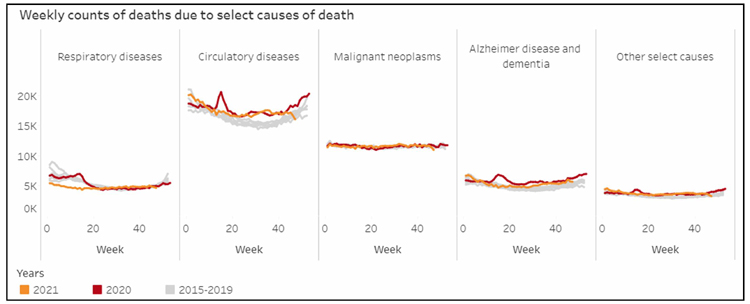
This chart from the U.S. CDC shows the trend of deaths from various causes in the U.S. The current year, 2021 (yellow line), remains essentially in line with the previous five year baseline. Meanwhile, this same CDC database shows huge surges in excess deaths in late winter and Fall of 2021 (see chart page one) that are not present in this Causes of Death chart. These excess deaths could be COVID-19 “vaccine” deaths that the CDC simply chose not to count as a select cause in this database chart in order to hide the severity of the numbers. YouTube recently deleted this writer’s video showing this data. chart: https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm#dashboard
The CDC also tracks yearly deaths from select causes (not just COVID) in the U.S. by the week. The surges in 2020 excess deaths were reflected in the 2020 select cause of deaths charts. You can see these surges represented in the red line of these charts corresponding with the 2020 excess death surges (see charts, this page). However, the CDC's cause of death charts intriguingly do not show any corresponding peak in deaths during the two surges of 2021. Notice how the yellow lines, which represent 2021 are essentially flat compared to the gray lines five year baseline representing 2015 thru 2019. There are no peaks in any of the 2021 select causes of death which coincide with the two massive excess deaths peaks the CDC shows in their excess deaths chart, leading people to wonder what were the actual causes of those excess deaths in 2021. A four minute video of the information in the above paragraphs was produced by this writer and posted on YouTube, citing all CDC links and asking the rhetorical question if the excess deaths could be from the ’vaccines.’ It was deleted by YouTube in less than 24 hours for “medical misinformation.” The video is, however, archived on this writer’s Rumble channel, the link is in footnote number 7, in the endnotes section of this article. The 2021 VAERS database shows the most COVID ‘vaccine’ deaths in the 75+ age group (6,581), followed by the 65 - 75 year age group (2,850) but more than 7,500 death entries do not specify an age at all. It also shows 40 vaccine deaths in children up to 17 years of age. This lower number is likely due to the fact that the ‘vaccines’ haven’t enjoyed Emergency Use Authorization for those age groups for as long as the adult group and that many parents are hesitant at enrolling their children in those medical trials given their concern for their children’s safety due to the known risks, such as heart issues and blood clotting, associated with the experimental shots now being found in that younger age group.
As of December 3, 2021 the VAERS total death reports show Pfizer’s ‘vaccine’ with the highest number (13,268) followed by Moderna (4,894) and Janssen (1,651) and 73 deaths for an undisclosed vaccine brand name.10
Dr. Stephanie Seneff, Ph. D. is a senior research scientist at Massachusetts Institute of Technology (MIT) and has been conducting research there for over fifty years, spending a large portion of her career investigating hazards and mechanisms of glyphosate, commonly found in weed killers. However, she diverted her research to the novel mRNA gene transfer technologies in early 2020, when “Operation Warp Speed” was announced by President Trump. In May, 2021, Dr. Seneff published a research paper with Dr. Greg Nigh in the International Journal of Vaccine Theory, Practice and Research entitled, “Worse than the Disease? Reviewing Some Possible Unintended Consequences of the mRNA Vaccines Against COVID-19.”8
In their paper, the two doctors noted all of the unprecedented aspects of the COVID-19 ‘vaccine’ development which should have set off alarm bells in the general community [editor: but weren’t, due to the establishment media’s pro-vaccine propaganda campaign being waged on behalf of their pharmaceutical company sponsors.]
Drs Seneff and Nigh noted these brand new vaccines were the first in many categories, such as:
1.) First to use PEG (polyethylene glycol) in an injection;
2.) First to use mRNA vaccine technology against an infectious agent;
3.) First time Moderna has brought any product to market;
4.) First to have public health officials telling those receiving the vaccination to expect an adverse reaction. [emphasis in original]
5.) First to be implemented publicly with nothing more than preliminary efficacy data;
6.) First vaccine to make no clear claims about reducing infections, transmissibility, or deaths;
7.) First coronavirus vaccine ever attempted in humans;
8.) First injection of genetically modified polynucleotides in the general population.
There are many problems with the alleged vaccines, from the artificial spike proteins causing blood clots to an overall reduction in the immune system’s capability all the way to in increase in prion diseases.
Dr. Joseph Mercola, M.D. recently interviewed Dr. Seneff about the alleged COVID ‘vaccines.’ “[She] said, ‘To have developed this incredibly new technology so quickly, and to skip so many steps in the process of evaluating [its safety], it’s an insanely reckless thing that they have done. My instinct was that this is bad, and I needed to know [the truth],’” recalls Dr. Mercola in a recent paper entitled Unintended Consequences of mRNA Shots.9 “Seneff suspects that in the next 10 to 15 years, we’ll see a dramatic spike in prion diseases, autoimmune diseases, neurodegenerative diseases at younger ages, and blood disorders such as blood clots, hemorrhaging, stroke and heart failure.”
A September 25, 2021 pre-print study entitled “Comparison of adverse events between COVID-19 and Flu vaccines”10 looked at the many adverse events of the COVID ‘vaccines.’ The researchers found a 16 times greater incidence of myocarditis (dangerous heart inflammation) in 12-15 year olds over the seasonal flu vaccine. They also found a 20 times greater incidence of visual changes in that age group using the Pfizer product compared to the number of events that occur for them in flu vaccines. For older age groups they found central and peripheral neuropathy (nerve damage) occurred at 30 to 100 times greater rates in the COVID vaccines when compared to flu vaccines.
The COVID-19 injections appear to be the wrong application for fighting a respiratory virus. As Dr. Mercola notes, “Normally you breathe the virus in and stimulate the production of IgA antibodies that protect your respiratory system. When you bypass that route of exposure with a jab in the arm, no secretory IgA antibodies are produced, leaving you susceptible to the infection.” Dr. Mercola explains the problem with circumventing the frontline immune response found in the respiratory system with a shot that bypasses it and puts the vaccine directly into the bloodstream, “In the end, your body will essentially believe your innate immune system failed, which means it must bring in the backup cavalry. In essence, your body is now overreacting to something that isn’t true. You’re not actually infected with a virus and your innate immune system has not failed, but your body is forced to respond as if both are true.”
This excessive over-response can then overwork the immune system and cause it to “play itself out” thus opening the person up to infections from other sources that they would have been able to fend off if they hadn’t received the experimental gene therapy shot to begin with.
Ronald Kostoff explained in a December 8, 2021 article at Trial Site News entitled “The Wrong Bomb Over the Wrong Target at the Wrong Time”11 that, “An effective vaccine would focus on cellular immunity in the respiratory and intestinal tract, in which secretory IgA is produced by your lymphocytes that are located directly underneath the mucous membranes that line the respiratory and intestinal tract. The antibodies produced by these lymphocytes are ejected through and to the surface linings. These antibodies are thus on site to meet air-borne viruses and they may be able to prevent viral binding and infection of the cells. Unfortunately, the main inoculants used presently for COVID-19 focus on antibodies (IgG and circulating (IgA) that occur in the bloodstream. These antibodies protect the internal organs of the body from infectious agents that try to spread via the bloodstream. A natural infection with SARS-CoV-2 will in most individuals remain localized to the respiratory tract. The vaccines used presently cause cells deep inside the body to express the viral spike protein, which they were never meant to do by nature. Any cell which expresses this foreign antigen on its surface will come under attack by the immune system, which will involve both IgG antibodies and cytotoxic T-lymphocytes. This may occur in any organ, but the damage will be most severe in vital organs. We are seeing now that the heart is affected in many young people, leading to myocarditis or even sudden cardiac arrest and death. In other words, we are dropping the wrong bomb over the wrong target at the wrong time.”
The takeaway here is that the experimental COVID-19 gene therapy ‘vaccines’ are causing a considerable amount of harm in the short-term, but the long-term effects—which were never studied previously—may play out in the future by devastating the health and livelihood of the global population who agreed to submit to these experimental medical trials unwittingly believing they were going to receive some form of immunity to a virus which has the survival rate of seasonal flu.
notes
1. https://medalerts.org/vaersdb/findfield.php?TABLE=ON&GROUP1=AGE&EVENTS=ON&VAX=COVID19&DIED=Yes
2. https://wonder.cdc.gov/vaers.html (I have a printout of that data request if you want a copy)
3. https://www.cdc.gov/mmwr/volumes/70/wr/pdfs/mm7034e5-H.pdf
4. https://www.sciencedirect.com/science/article/pii/S221475002100161X
5. https://stevekirsch.substack.com/p/latest-vaers-estimate-388000-americans
6. https://www.cdc.gov/nchs/nvss/vsrr/covid19/excess_deaths.htm#dashboard
8. https://ijvtpr.com/index.php/IJVTPR/article/view/23
10. https://www.medrxiv.org/content/10.1101/2021.09.22.21263711v1.full.pdf
11. https://trialsitenews.com/covid-19-vaccines-the-wrong-bomb-over-the-wrong-target-at-the-wrong-time/