Back to Fort Fairfield Journal WFFJ-TV Contact Us
COVID-19 Survival Rate Rises as Mainstream Media & Governments Attempt to Perpetuate Coronavirus Hype
Takedown of Western Civilization Now in Full Swing

Presque Isle Main Street is eerily quiet during the 4pm-5pm rush hour on March 30. In the midst of a fourteen day state mandated shutdown of all “non-essential” businesses, Presque Isle - a city of 12,000 overnight which expands to nearly 20,000 during daily business hours - has become desolate with only grocery stores, auto parts stores and a few other “essential” businesses allowed to remain open. The shut-down is supposed to end on April 8, but considering President Trump has extended social distancing guidelines until April 30, Maine’s governor, Janet “Big Sister” Mills has extended the ban on all non-essential businesses and issued a stay at home order for everyone not deemed "essential" through April 30. photo/David Deschesne
By: David Deschesne
Fort Fairfield Journal, April 1, 2020
The novel coronavirus, COVID-19 exploded in the United States over the past two weeks garnering breathtaking attention from the mainstream media with wall-to-wall coverage exuding every possible minute detail and statistic. Updated COVID-19 world maps, maps of the U.S. and each U.S. state’s respective maps of their counties detailed a daily dose of statistics for “cases,” “deaths” and “hospitalizations” from the virus.
But, amidst all the noise and hoopla, it was lost on most people that, as of the time of this writing, the outbreak isn’t any more severe than the seasonal flu; in many places, it is much less. Reports kept touting “total case numbers” with recoveries buried in the data since they weren’t deemed as sensational enough; leaving it up to the readers to do the math themselves to determine actual active cases after the recovered victims were factored out of the equation.
The seasonal flu afflicts on average, 60 million U.S. inhabitants per year, and its complications kill 22,000 to 55,000 people per year in the U.S. alone. Rochester Regional news reports that as of March 7, 2020 the CDC estimates there have been 45 million conventional flu illnesses in the U.S. so far this flu season, with 300,000 hospitalized and over 46,000 deaths (over 83,000 flu deaths for the entire 2019-20 flu season). Contrast that with the 177 thousand verified COVID-19 cases across the U.S. and its death rate of only around 3,400 as of March 30 and it’s curious why we’re not seeing exhaustive maps and daily updates on flu cases and flu deaths spurned out by various State governments then incessantly parroted by the mainstream media. Certainly, schools aren’t closed and the entire economic infrastructure of the country shut down for a typical flu outbreak which can be on an order of magnitude many times more destructive than the current COVID-19 coronavirus.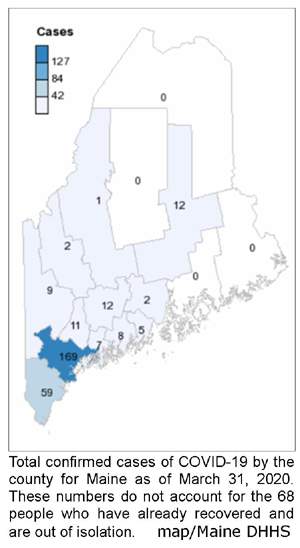
Maine had a lackluster showing on the national COVID-19 scoreboard in the opening quarter of the game. At the end of March, there were only around 235 active, confirmed cases of COVID-19 in the entire state, after subtracting out those who were confirmed to have the virus but had fully recovered. Over 3,800 tests for COVID-19 came back as “negative.”
At the end of March, four counties out of the sixteen in Maine didn’t even have a confirmed COVID-19 case; though in hindsight, some people in those locations believed they might have had the virus before all the media hype, but then recovered from it before test kits were readily available.
Maine is following the national trend in other demographics, though. For example, population dense centers like Portland - which is essentially a suburb of Boston - had impressive case numbers along with all the rest of the major U.S. cities and dense population centers. Meanwhile, sparsely populated Aroostook County at the other end of the State was one of the four at the end of March with no cases reported.
One of the primary strategies to prevent the spread of the virus was to shut down all schools and businesses and keep everyone home - a tactic borrowed from the last major flu epidemic of the early 1900’s. The data, however, does not completely support that strategy. By keeping people home in enclosed spaces with other family members actually increase the chances of infected members spreading it among themselves.
According to Dr. Paul Auwaerter, the Clinical Director for the Division of Infectious Diseases at Johns Hopkins University School of Medicine, “If you have a COVID-19 patient in your household, your risk of developing the infection is about 10%...If you were casually exposed to the virus in the workplace, your chance of infection is about 0.5%.”
In an op-ed on nationalpost.com, Stanford University Professor of Medicine and Professor of Epidemiology and Public Health, John P.A. Ioannidis points out the problems of using insufficient data with school closures due to COVID-19; “In the absence of data, prepare-for-the-worst reasoning leads to extreme measures of social distancing and lockdowns. Unfortunately, we do not know if these measures work,” writes Prof. Ioannidis. “School closures, for example, may reduce transmission rates. But they may backfire if children socialize anyhow, if school closure leads children to spend more time with susceptible elderly family members, if children at home disrupt their parents ability to work, and more. School closures may also diminish the chances of developing a herd immunity in an age group that is spared serious disease.”
Prof. Ioannidis goes on, “One of the bottom lines is that we don’t know how long social distancing measures and lockdowns can be maintained without major consequences to the economy, society and mental health. Unpredictable evolutions may ensue, including financial crisis, unrest, civil strife, war, and meltdown of the social fabric.”
“The response has not been modern and scientific,” wrote Jeffrey Tucker from aier.org. “It has been medieval and mystical. The theory behind the policy has been nothing but a panicked cry of run and hide before the noxious gas gets you. Lacking reliable data - which is the fault of the CDC and FDA - we replaced knowledge with power.”
In the run-up to the outbreak of COVID-19 in the U.S., media consumers watched with horror as the death rate soared in Italy. What was lost in that discussion, though was the fact that society in Italy is structured differently than the U.S. In Italy, for example, it is not uncommon for three to four generations of a family to live under one roof. The elderly there are also more active and tend to get outside and socialize with each other much more than their U.S counterparts. This helped to spread the virus among family members for sure. In Italy, most of those infected were over the age of 60, but the median age of fatality was 80 years. Of all the fatalities in Italy under the age of 40, it was shown they were males with serious pre-existing medical conditions.
But, the deaths attributed to COVID-19 are among people who were already suffering long-term medical issues such as cancer, COPD, emphysema, etc which may have been the actual cause of death. This is how the numbers are being gamed to support lockdown of society.
In Spain, the death rate was also elevated. But, this could be due to substandard sanitary conditions within the health care field. There were reports that nursing home staff in Spain were leaving COVID-19 death victims in their beds for several hours before getting around to removing them.
Ergo, using the Italian or Spanish models to predict the outcome of a similar viral outbreak in a completely different society - like the U.S. - would create a scenario riddled with errors - as seen with the most recent numbers and demographics. Such hyped up media reports may have lead to some overreaction in the U.S.
“Local governments and politicians are inflicting massive harm and disruption with little evidence to support their draconian edicts,” said researcher, Aaron Ginn in a report posted on the economic website, zerohedge.com. “Every local government is in a mimetic race to one-up each other in authoritarian city ordinances to show us who has more ‘abundance of caution.’ Politicians are competing, not on more evidence or more COVID-19 cures but more caution. As unemployment rises and families feel unbearably burdened already, they feel pressure to ‘fix’ the situation they created with even more radical and ‘creative’ policy solutions. This only creates more problems and an even larger snowball effect. The first place to start is stop killing the patient and focus on what works.”
In addition to a healthy dose of mainstream media hype, government officials - who are people, too, with all the same fears and anxieties as the rest of society - likely read a report from Imperial College in London, headed up by Neil M. Ferguson. In the report, entitled, Impact of non-pharmaceutical interventions (NPIs) to reduce COVID-19 mortality and healthcare demand, the authors used computer models to war-game a virtual scenario that showed COVID-19 ramping up in the U.S. around mid-April and death rates, hospital stays and state-wide quarantines lasting for three to five months - out to perhaps 18 months when a vaccine might finally be developed. But how trustworthy is the model? This is the same crowd that bungled the predictions on Foot and Mouth disease in 2001 and the H1N1 Swine Flu in 2009. Yet, governments still listen to them and take them seriously. Imperial College’s whole COVID-19 report was simply an academic exercise, with variations of the disclaimer phrase, “we assume” appearing multiple times on each page of the twenty-page report. The report painted a bleak picture, predicting 510,000 total deaths in the U.K. and 2.2 million in the U.S. from April thru August. Current statistics, however, derived from numbers within the U.S. do not support the conclusions of that report. RT reports Professor Ferguson revised his 510,000 UK death figure down to at most 20,000. More recently he revised them down further to just 5,700. “One wonders what happened to change his mind,” writes Peter Andrews from RT. “It seems that the lower than expected mortality rates are causing experts to re-evaluate their more apocalyptic predictions.”
But the initial reaction by government leaders to reports like Ferguson’s created a nearly panicked adoption of all sorts of tactics to slow a benign virus which predominately spreads among people in long-term contact with each other in enclosed spaces, such as homes.
Social distancing, business closures, school closures, in-home quarantines statewide and even plexiglass “cough barriers” installed at checkouts throughout major stores deemed essential enough to stay open were just some of the reactions to COVID-19 which were never before deployed for the conventional seasonal flu which annually infects and ultimately kills many thousands more people than this current coronavirus has thus far.
Maine’s numbers at the end of March mark five deaths out of the 303 confirmed COVID-19 cases with 68 recoveries. This amounts to about a 1.6% fatality rate. Most of these cases were in the age of 60 - 80 years. The Maine CDC has not released information regarding the victims’ pre-existing health issues, so COVID-19 may not have been the actual cause of those deaths anyway.
The national average fatality from COVID-19 stands at around 1.8%. But, it could be much lower since most States are only factoring in those select high risk individuals who have been actually tested for the virus - which are people with high exposure, such as healthcare workers, or patients with severe symptoms and potentially bad outcomes to begin with. Given this fact, the death rate will obviously be artificially higher than it would be if all cases were factored in.
This numbers-skewing tactic was confirmed for Maine by Dr. Nirav Shah, director of the Maine CDC. In a webcast press conference on March 31, Dr. Shah said up to this point they had been prioritizing tests on the “highest risk” individuals and have been holding on to the samples from the “lower risk” individuals.
“These are samples that have been waiting at our laboratories but, because of our focus on the highest risk individuals, have not yet been tested,” said Dr. Shah. “As of right now that number stands at 600 tests. These represent individuals that were in the lowest risk category. As of right now, individuals in the highest risk category - individuals hospitalized, healthcare workers, or folks from congregate settings - there is no backlog of tests at the Maine State lab in Augusta.”
When factoring in all of the people who actually have, or have had, the COVID-19 virus - which may be impossible data to obtain at this point - and considering most of them do survive, the death rate could plummet to well below one percent. Some estimates put it as low as 0.45%
Hospitalization rates in Maine were also low. Out of the first 150 or so verified cases in Maine, only 22 people were in bad enough shape to require hospitalization. The rest of them simply rode out the virus and recovered while quarantined at home.
To be fair, COVID-19 could still be a problem. With U.S. hospitals already functioning at near capacity with the flu and all the other illnesses they have to deal with, an additional influx of even a moderate COVID-19 outbreak could send them over their tipping point as intensive care units (ICUs), ventilators and beds come into short supply.
On March 31, President Trump kicked the can further down the road by extending the federal social distancing guidelines until the end of April. Maine’s governor, Janet “Big Sister” Mills has extended the ban on all non-essential businesses and issued a stay at home order for all non-essential employees through April 30.
March 25, 2020 – Governments and Media Pushing to Collapse Entire U.S. Society With Coronavirus Scare